
Margeaux Cannon, PhD • December 8, 2025
You can reclaim your life from OCD and anxiety with ERP therapy.
If you’ve ever struggled with intrusive thoughts, anxiety, or compulsive behaviors, you may have come across ERP—short for Exposure and Response Prevention.
ERP is widely regarded as the gold standard for treating OCD and is increasingly being used to treat other anxiety-related conditions. This article provides an overview of ERP, including what it is, how it works, who it helps, and what to expect from the process.
What is Exposure and Response Prevention (ERP)?
Exposure and Response Prevention is a specific type of Cognitive Behavioral Therapy (CBT) designed to help individuals confront their fears rather than avoid them, resist them, or neutralize them with rituals or compulsions. It has two main components:
- Exposure: Gradually and intentionally facing the things that cause fear or discomfort. Imaginary exposures include thoughts, mental images, and stories. In vivo exposures include real-life situations and experiences. Interoceptive exposures include physical sensations.
- Response Prevention: Refraining from performing the compulsive behavior or mental ritual typically used to reduce the distress associated with the obsession.
Compulsive behaviors can include tapping, washing, checking, asking for reassurance, or doing things a particular way. Compulsive behaviors can also include avoiding doing things including avoiding touching doorknobs, driving, and talking.
Mental rituals can include silent counting, replaying memories, comparing, and mantras.
By repeatedly facing fears and resisting compulsions, the brain learns that the anxiety decreases on its own and that feared outcomes are less likely or not as catastrophic as once believed.
The Science Behind ERP
Anxiety and OCD often work cyclically. We experience a trigger, which cues an obsession or intrusive thought. If our brain interprets the trigger or thought as threatening, our threat-response system (also known as the
sympathetic nervous system or
fight or flight) activates. The threat-response system can lead to emotional and physical distress, including symptoms like increased heart rate.
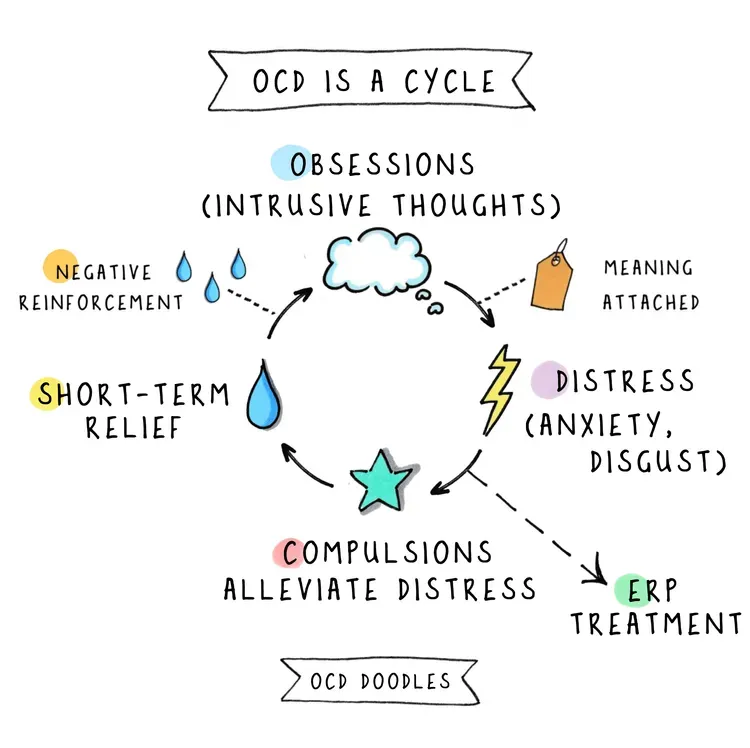
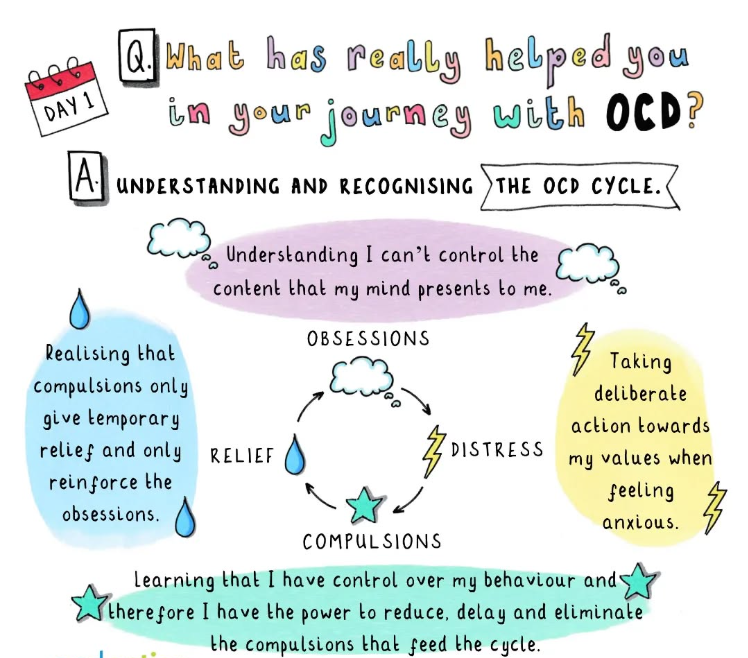
We might attempt to reduce the threat to alleviate our distress. Sometimes that means solving the problem, avoiding the problem, or some other action or mental act that leads to short-term relief. The relief that we feel convinces us that the threat was real and the compulsion or avoidance was necessary. The relief reinforces future anxiety, which drives more avoidance and compulsions, and the cycle continues.
Unfortunately, we don’t actually have the ability to control whether bad things happen. We cannot control the future - bad things may or may not happen, no matter how careful and controlled we try to be. In addition, avoiding discomfort makes our worlds smaller and doesn’t give us opportunities to feel brave and resilient. While we are getting pushed around by our fears and trying to keep ourselves safe and comfortable, we miss out on the beautiful parts of life that require some uncertainty, discomfort, and effort. We also miss out on learning that we can do hard things, learn, and grow. We gain confidence by persevering through tough times.
“We can choose courage or we can choose comfort, but we can't have both. Not at the same time.”
-Brené Brown
ERP interrupts the anxiety cycle by giving us tools and experience to build motivation to face our fears. ERP helps us to stop doing things that bring us temporary relief and fuel more anxiety. By accepting short-term uncertainty and discomfort, we can get more comfortable with being uncomfortable and uncertain.
ERP is rooted in the principles of behavioral psychology, particularly the concept of habituation. Habituation refers to the natural decrease in anxiety that occurs when a person is exposed to a feared stimulus over time without engaging in avoidance or compulsions. This retrains the brain to respond more appropriately to anxiety triggers - we learn through experience that we can survive it and we don’t need to be as afraid of it. It’s like the difference between watching a scary movie alone in the dark for the first time versus watching a scary movie with the lights on for the tenth time. It’s just not as scary after you’ve done it several times without hiding from it.
Research consistently shows that ERP is one of the most effective treatments for OCD, with success rates as high as 60% to 80% when done correctly and consistently. Brain imaging studies have even shown structural and functional changes in the brains of people who undergo ERP, indicating long-term benefits.
Conditions Treated with ERP
While ERP is most commonly associated with OCD, it is also effective for a range of anxiety disorders and related conditions, including:
- Social Anxiety Disorder
- Panic Disorder
- Generalized Anxiety Disorder (GAD)
- Specific Phobias
- Health Anxiety (Hypochondria)
- Body Dysmorphic Disorder (BDD)
- Post-Traumatic Stress Disorder (PTSD), in some cases
ERP can be tailored to a wide variety of OCD subtypes. Some common themes include:
- Contamination OCD: Fear of germs, illness, or dirt
- Harm OCD: Fear of causing harm to oneself or others
- Sexual or Religious OCD: Intrusive taboo thoughts
- Checking OCD: Repeatedly checking appliances, doors, or personal mistakes
- Symmetry and Ordering OCD: Needing things to be “just right”
- Scrupulosity: Religious or moral obsessions
- Relationship OCD: Obsessive doubts about relationships
Each theme may involve different triggers and compulsions, but the underlying treatment principle remains the same: exposure to the feared thought or situation, followed by response prevention.
The ERP Process: What to Expect
- Assessment and Planning A therapist will begin with a detailed assessment to understand the individual’s specific fears, obsessions, and compulsions. This helps create a personalized ERP plan.
- Building Motivation The individual and therapist will work together to clarify and build the client’s motivation to engage with ERP. Because ERP includes facing fears and feeling uncomfortable, it’s important for the client to have a clear idea of what they really care about.
- Creating a Fear Hierarchy Together with the therapist, the individual will list their feared situations and rank them from least to most anxiety-provoking. This is called a fear hierarchy, and individuals and therapists use them to choose exposures. Usually, exposures begin with situations in the middle of the fear hierarchy.
- Gradual Exposure The individual begins confronting their fears in real-life or imaginal situations with the therapist. This can involve touching a doorknob without washing hands, imagining a distressing thought, breathing through a straw to experience shortness of breath that often comes with anxiety, or resisting the urge to check something.
- Response Prevention During and after exposure, the individual resists performing any compulsions. This is challenging but essential for the therapy to work.
- Repetition and Practice Exposures are repeated frequently until the anxiety subsides. Over time, new exposures are faced, and the individual works their way around the hierarchy.
- Maintenance and Relapse Prevention Once significant progress is made, the focus shifts to maintaining gains and developing strategies to prevent relapse.
Challenges and Misconceptions
ERP is highly effective, but it is not always easy. Some common challenges include:
- Initial Increase in Anxiety: Facing fears head-on can temporarily raise anxiety levels. It can help to think of this as a transition phase: change is often hard! It’s like when we want a more satisfying relationship or job - we need to do the hard work of acknowledging the problem and then persevering through the changes to get what we really want.
- Avoidance or Resistance: It’s common to want to avoid exposures or give in to compulsions. Of course you might not WANT to do the hard thing or feel the uncomfortable feeling. The therapist and client can work together to build motivation by remembering how life could be better without OCD in control.
- Misunderstanding the Process: Some people fear that ERP is about forcing them into extreme situations too quickly. In reality, ERP is gradual and collaborative. Consent and choice is a crucial part of the process.
Misconceptions can deter people from trying ERP. For instance, it’s not about ignoring fears but confronting them with support. It also doesn’t require 100% certainty or perfection; rather, it teaches tolerance of uncertainty.
The Role of the Therapist
A skilled ERP therapist plays a critical role in guiding the process, providing support, and ensuring that exposures are done correctly and safely. They help tailor the approach to the individual's needs and adjust the plan as therapy progresses.
A key to ERP is personal motivation. Therapists can help clients stay engaged and motivated during exposures by answering these questions.
- What would life look like without this issue?
- Why does this matter to you?
- What is anxiety and OCD keeping from you?
- Why would you do this hard thing and keep going?
- What do you have to gain from doing this?
Therapists can help you to become your own cheerleader and coach by encouraging yourself through the exposures.
- “I can do hard things.”
- “I can feel uncomfortable and still be okay.”
- “I am resilient.”
- “I believe in myself.”
- “I am stronger than my anxiety/OCD.”
- “I’m being brave!”
Your therapist may encourage you to write or record your own helpful reminders and encouragement. These personalized phrases can be used to support you through the discomfort that may come from resisting compulsions.
Other Possible Benefits from ERP
In addition to reducing the severity and frequency of OCD and anxiety symptoms over time, ERP can help us in other areas of life. If we embrace the “I can do hard things” mindset, we may have an easier time being open to new experiences, letting go of control, and coping with unexpected situations. Some clients who engage with ERP find that they become less perfectionistic and controlling, even though that was not what initially brought them to therapy.
Self-Help and Digital Tools
While working with a therapist is ideal, some people begin with self-help resources or use digital tools to complement therapy. These include:
- Books: "Freedom from Obsessive Compulsive Disorder" by Jonathan Grayson, or "The OCD Workbook" by Bruce Hyman.
- Apps and websites: NOCD, WorryTree, and
anxieties.com
- Social Media: @ocddoodles
Conclusion: Reclaiming Life Through ERP
Exposure and Response Prevention is more than just a treatment; it is a transformative process that empowers individuals to reclaim their lives from the grip of anxiety and OCD. While it can be challenging, the results are often life-changing. With commitment, support, and the right guidance, ERP helps people confront what they fear most and discover that they can handle it—often with greater strength than they ever imagined. The path may not be easy, but it is one grounded in hope, resilience, and proven success.
You can begin your path to recovery at Aviva Psychology Services by filling out the Request an Appointment form. Our admin team will contact you quickly to arrange scheduling.
References
Abramowitz, J. S. (2009). The family guide to getting over OCD: Reclaim your life and help your loved one. The Guilford Press.
Foa, E. B., Yadin, E., & Lichner, T. K. (2012). Exposure and response (ritual) prevention for obsessive-compulsive disorder: Therapist guide (2nd ed.). Oxford University Press.
Grayson, J. (2014). Freedom from obsessive compulsive disorder: A personalized recovery program for living with uncertainty (2nd ed.). Berkley Books.
Hyman, B. M., & Pedrick, C. (2010). The OCD workbook: Your guide to breaking free from obsessive-compulsive disorder (3rd ed.). New Harbinger Publications.
Kozak, M. J., & Foa, E. B. (1997). Mastery of obsessive-compulsive disorder: A cognitive-behavioral approach—Therapist guide. Oxford University Press.
National Institute of Mental Health. (n.d.).
Obsessive-Compulsive Disorder. https://www.nimh.nih.gov/health/topics/obsessive-compulsive-disorder-ocd
SHARE THIS POST:
Our Recent Posts:






